Ischiofemoral Impingement (IFI)

Ischiofemoral impingement (IFI) was first reported by Dr. Kenneth Johnson in 1971 in three patients with hip pain following hip replacement surgery. Each patient presented with pain that was increased with adduction (bringing the leg across the body) of the extended hip. Radiographs revealed narrowing between the ischium and lesser trochanter, with enlargement of the lesser trochanter. It was concluded that the pain was “due to a pinching of soft tissues between bone prominences”. Due to failure of non-surgical management, each patient underwent surgical excision of the lesser trochanter with complete relief of pain.
Beginning in 2008, IFI has been rediscovered as a source of hip, groin, and/or posterior (back of the leg) thigh pain. Prior to that time, edema signal intensity on MR within the quadratus femoris muscle (QFM) was attributed to muscle strains. Using MR, it has been recognized that a narrowed ischiofemoral space may cause impingement or compression of the QFM, resulting in muscle edema and, over time, muscle atrophy. On examination, pain is elicited with various hip motions, including extension of the leg and a long stride in walking.
Quadratus femoris, Latin for “square muscle of the thigh,” is a quadrilateral-shaped muscle located between the lesser trochanter of the proximal femur and the ischial tuberosity, around the back of the hip. A bursa may be found between this muscle and the lesser trochanter. The QFM is bordered anteriorly by the obturator externus muscle, posteriorly by the sciatic nerve, superiorly by the inferior gemellus muscle and inferiorly by the adductor magnus muscle.
The QFM is one of the short rotator muscles of the hip along with the piriformis, superior and inferior gemellus, and obturator internus and externus muscles. It is a strong external rotator of the hip and thigh that assists with adduction.

Normal anatomy of the ischiofemoral space
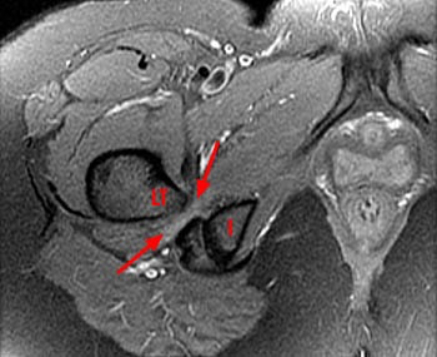
Patientient with a narrowed space (shown by the arrows)
(I: Ischium (sit bone); LT: Lesser trochanter)
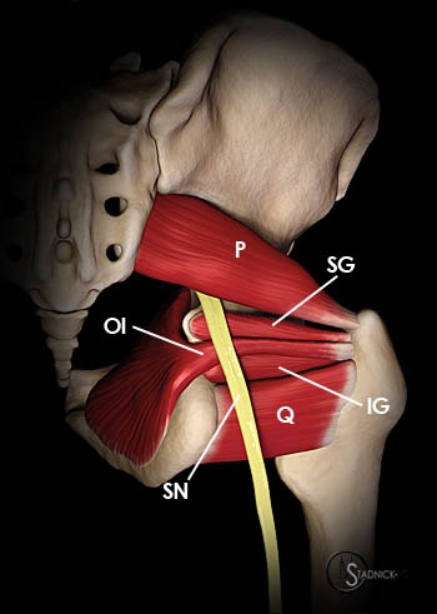
Figure above shows the relationship of the sciatic nerve to the area of possible entrapment. (SN: Sciatic nerve; Q: Quadratus femoris; OI: Obturator internus: IG: Inferior gemellus; SG: Superior gemellus; P: Piriformis.
Clinical Presentation
IFI typically occurs in middle-aged to elderly women and is uncommon in males. Both hips are involved in 25-40% of patients. Most patients have hip and/or groin pain. Shooting pain to back of the thigh and knee is not uncommon and is likely due to irritation of the adjacent sciatic nerve. Chronic low back pain is common and may prompt an MRI of the lumbar spine as the first advanced imaging test performed. Many patients first see a spine surgeon since the symptoms are very similar to those of patients with ongoing back problems. Patients may report a snapping sensation, locking of the joint and noise in the joint. On examination, most patients have pain with hip range of motion. Symptoms may be reproduced by a combination of hip extension, adduction and external rotation or with flexion and internal rotation. This pain is usually located in the back of the hip or buttocks.
Imaging Features
In patients with IFI, radiographs are usually normal but may show abnormal space between the ischium (sit bone) and lesser trochanter (a prominence in the back of the thigh bone, near the hip joint). MRI is used to assess the size and signal intensity of the QFM and the space available for this muscle between the ischium and thighbone.
On MRI, the QFM demonstrates edema, centered on the muscle belly, at the site of maximal impingement. With increased severity of impingement, edema becomes more severe and diffuse and may involve the surrounding soft tissue.
On xrays, the space between the ischium (sit bone) and the thigh bone is significantly more narrow than normal. In patients with IFI, this narrowing has been reported on both side in 25-40. Also, most patients (84-100%) are female. This is likely due to the female pelvis having greater width and smaller depth with the sit bones further apart. This impingement process can be demonstrated on a cadaver.
Other problems that may feel similar to the patient and may be ruled out by you physician include tendinitis, hamstring injury, snapping hip syndrome, piriformis syndrome and a nerve problem emanating from the back. A stress fracture of the hip can also have similar features.
Piriformis syndrome is a rare, controversial clinical problem in which buttock and hip pain are attributed to entrapment of the sciatic nerve by the piriformis muscle at the greater sciatic notch (see first figure). Potential reasons include an enlarged piriformis muscle, a constricting fibrous band, sometimes the sciatic nerve can go through the piriformis muscle, rather than under it. MRI of the pelvis has shown potential in evaluating this syndrome but a large series of patients has not been studied due to the rarity of the problem.
Other problems that can appear to be similar to your physician include acetabular labral tear, femoroacetabular impingement, athletic pubalgia, osteitis pubis, avascular necrosis, pelvic inflammatory disease and hernias. In middle-aged and elderly women (the typical patient with IFI), stress fracture is an important cause of hip or groin pain and MR is usually relied upon for diagnosis.
Treatment
No definitive treatment strategy for IFI has been established. Initial treatment is conservative and includes rest, activity restriction and non-steroidal anti-inflammatory drugs. Ultrasound-guided infiltration of the QFM with local anesthetic and steroid has been reported to provide long-lasting pain relief. For patients who do not respond to conservative management, surgical excision of the lesser trochanter and removal of reactive or bursal-type tissue has been performed without reports of complication. In some situations endoscopic (or minimally invasive) decompression of the ischiofemoral space may be a feasible approach, as described in this chapter.